What to Expect After Microdiscectomy or ACDF: A Recovery Timeline
Quick Answer
Cervical disc replacement preserves neck motion while ACDF fusion eliminates it at the treated level. Both procedures relieve arm pain from nerve compression with similar 85–outcomes vary by diagnosis and patient factorss. CDR is preferred for younger active patients with healthy facet joints; ACDF is better for facet arthritis, instability, or multilevel disease. Dr. Greenberg at Greenberg Spine in Fort Wayne evaluates both options and recommends based on your specific anatomy and imaging.
A Fort Wayne Guide to Cervical Spine Surgery Options

Understanding Your Options
When cervical disc disease causes persistent arm pain, numbness, or weakness, two main surgical options exist: cervical disc replacement (CDR) and anterior cervical discectomy and fusion (ACDF). Both effectively treat nerve compression, but they differ significantly in their approach to spinal motion.
The Procedures Explained
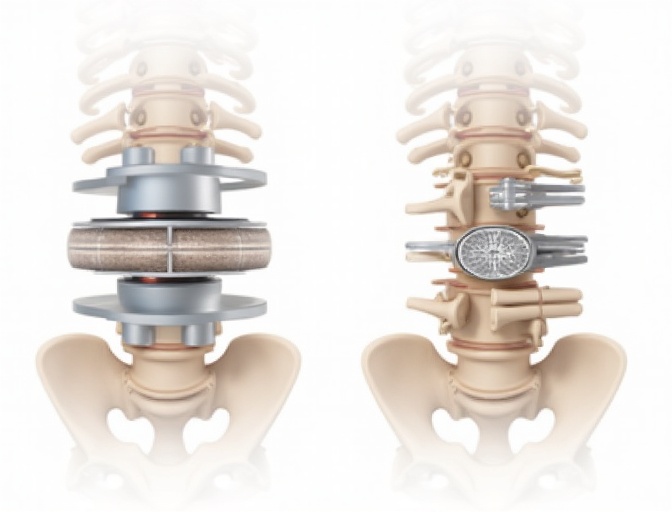
Cervical Disc Replacement
Removes the damaged disc and replaces it with an artificial disc designed to maintain natural neck motion.
- Preserves spinal motion
- May reduce adjacent level disease
- Faster return to activities
- No bone graft needed
ACDF (Fusion)
Removes the damaged disc and fuses the vertebrae together using a bone graft or cage, eliminating motion at that level.
- Time-tested, proven technique
- Long-term outcome depends on patient-specific factors
- Suitable for most conditions
- Lower revision rates
Why Choose Greenberg Spine?
Dr. Marc Greenberg brings fellowship-trained expertise in minimally invasive and motion-preserving spine surgery to Fort Wayne. Our evidence-based approach combines the latest surgical techniques with personalized patient care.
Motion Preservation: The Key Difference
Why Motion Matters
Cervical disc replacement maintains the natural movement of your neck, which may help prevent adjacent level disease—a condition where discs above or below a fusion develop problems over time.
With Motion Preservation:
- • Normal neck rotation and flexion
- • Reduced stress on adjacent levels
- • More natural biomechanics
- • Faster return to sports/activities
With Fusion:
- • Eliminated motion at treated level
- • Increased stress on adjacent discs
- • Potential for adjacent level disease
- • Permanent motion restriction
Recovery Timeline Comparison
| Recovery Milestone | Disc Replacement | ACDF |
|---|---|---|
| Hospital Stay | Same day or overnight | Overnight to 1-2 days |
| Collar Use | 1-2 weeks (comfort only) | 6-12 weeks (required) |
| Return to Work | 2-4 weeks | 4-6 weeks |
| Driving | 1-2 weeks | 2-6 weeks |
| Full Activities | 6-8 weeks | 3-6 months |
| Sports/Exercise | 8-12 weeks | 3-6 months |
Long-term Outcomes & Evidence
Clinical Studies Show:
- Similar pain relief and functional improvement
- Comparable patient satisfaction rates
- Both procedures highly effective for nerve compression
- 10+ year follow-up data available for both
Key Differences:
- CDR: Lower adjacent level disease rates
- ACDF: Lower revision surgery rates
- CDR: Maintained neck motion
- ACDF: More predictable outcomes
Who Is a Candidate?
Good Candidates for Disc Replacement:
- Single-level disc disease
- Healthy facet joints
- Good bone quality
- Age typically under 60
- Active lifestyle
- Normal neck alignment
- No significant arthritis
- Adequate disc height
ACDF May Be Better For:
- Multi-level disease
- Significant arthritis
- Spinal instability
- Previous neck surgery
- Kyphotic (reversed) alignment
- Osteoporosis
- Infection or tumor
- Facet joint disease
Risks & Considerations
Important Considerations
Both procedures carry similar surgical risks, but long-term considerations differ. Disc replacement may require future revision surgery, while fusion is generally permanent but may lead to adjacent level problems.
Disc Replacement Risks
- Device wear or failure (rare)
- Heterotopic ossification
- Potential for revision surgery
- Limited long-term data
ACDF Risks
- Adjacent level disease
- Pseudarthrosis (non-union)
- Permanent motion loss
- Graft-related complications
Making the Right Choice
The Decision Process
The choice between disc replacement and fusion depends on your specific anatomy, lifestyle, age, and goals. A thorough evaluation including imaging and physical examination helps determine the best option.
Medical Factors
Anatomy, bone quality, disc condition
Lifestyle Goals
Activity level, sports participation
Age & Longevity
Expected device lifespan, revision risk
Related Topics
Learn more about related conditions and treatments
About this content
This page was written and clinically reviewed by Marc Greenberg, MD, a fellowship-trained spine surgeon who trained at Mayo Clinic, Johns Hopkins, and Brown University, practicing in Fort Wayne, Indiana. Information is for educational purposes only and is not a substitute for medical advice from your physician.
Ready to Explore Your Options?
Schedule a consultation to determine which cervical spine procedure is best for your specific condition.
Related Information
Disclaimer: Information is educational, not medical advice. Outcomes vary. Individual results depend on many factors including age, health status, anatomy, and adherence to post-operative instructions. Always consult with a qualified spine surgeon for personalized medical advice.
Related Articles

Minimally Invasive vs. Open Spine Surgery: What's the Difference?
An educational comparison of minimally invasive spine surgery (MIS) and traditional open spine surgery. Covers what MIS means (smaller incisions, muscle-sparing tubular or endoscopic approaches), how open surgery differs (longer incision, muscle stripping), potential benefits of MIS in appropriate candidates (less tissue disruption, less blood loss, hospital stay planning, faster early recovery) using conditional population-level language, evidence on comparable long-term outcomes for appropriate procedures, candidacy factors (who may and may not be a candidate), and the supporting role of robotic guidance and navigation for surgical accuracy. Includes FAQ accordion with FAQPage JSON-LD. Internal links to minimally invasive, endoscopic, robotic procedure pages, condition pages, and the second-opinion page.
Disc Replacement vs. Fusion: Which Motion-Preserving Option Is Right for You?
Compare disc replacement vs. fusion for active adults. Fellowship-trained Fort Wayne spine surgeon Dr. Marc Greenberg explains motion preservation benefits, recovery timelines, and how to choose the right option.

Minimally Invasive Spine Surgery: What Indiana Patients Should Know
A patient-friendly educational guide to minimally invasive spine surgery (MIS) for Indiana patients. Covers what MIS actually means (a spectrum of techniques using smaller incisions and muscle-sparing approaches to achieve the same surgical goal), how it differs from traditional open surgery (comparison table covering incision size, muscle handling, blood loss, hospital stay, post-operative discomfort, and visualization), common conditions treated with MIS (herniated discs, spinal stenosis, spondylolisthesis, compression fractures, and degenerative disc disease — all with the caveat that surgery follows conservative care trial), what recovery looks like across four phases (immediate post-op, first two weeks, weeks 2-6, and longer-term with warning signs to call about), and practical guidance for accessing MIS care in Indiana and Northeast Indiana including the importance of fellowship training and starting with a consultation. Includes FAQPage JSON-LD, internal links to MIS overview, procedures, and related blog posts.