How to Choose a Spine Surgeon in Indiana: A Patient's Guide
Quick Answer
Balloon kyphoplasty is a minimally invasive procedure for painful vertebral compression fractures — most commonly from osteoporosis — that haven't improved with 4–6 weeks of conservative care. Dr. Marc Greenberg at Greenberg Spine in Fort Wayne performs kyphoplasty to restore vertebral height and relieve pain. Earlier intervention (within 4 weeks of fracture) is associated with better outcomes. Kyphoplasty treats the fracture but must be paired with bone health optimization to prevent future fractures.
A Fort Wayne Guide to Vertebral Compression Fracture Treatment

Who May Benefit from Kyphoplasty
Ideal Candidates
In appropriately selected acute/severe osteoporotic fractures with persistent pain and disability, randomized trials show faster pain relief and functional gains with balloon kyphoplasty compared with non-surgical care.
- Painful vertebral compression fractures (VCFs)
- Failed conservative treatment (4-6 weeks)
- Significant functional impairment
- Osteoporotic bone quality
Why Choose Greenberg Spine?
Dr. Marc Greenberg brings fellowship-trained expertise in minimally invasive and motion-preserving spine surgery to Fort Wayne. Our evidence-based approach combines the latest surgical techniques with personalized patient care.
Kyphoplasty vs Vertebroplasty
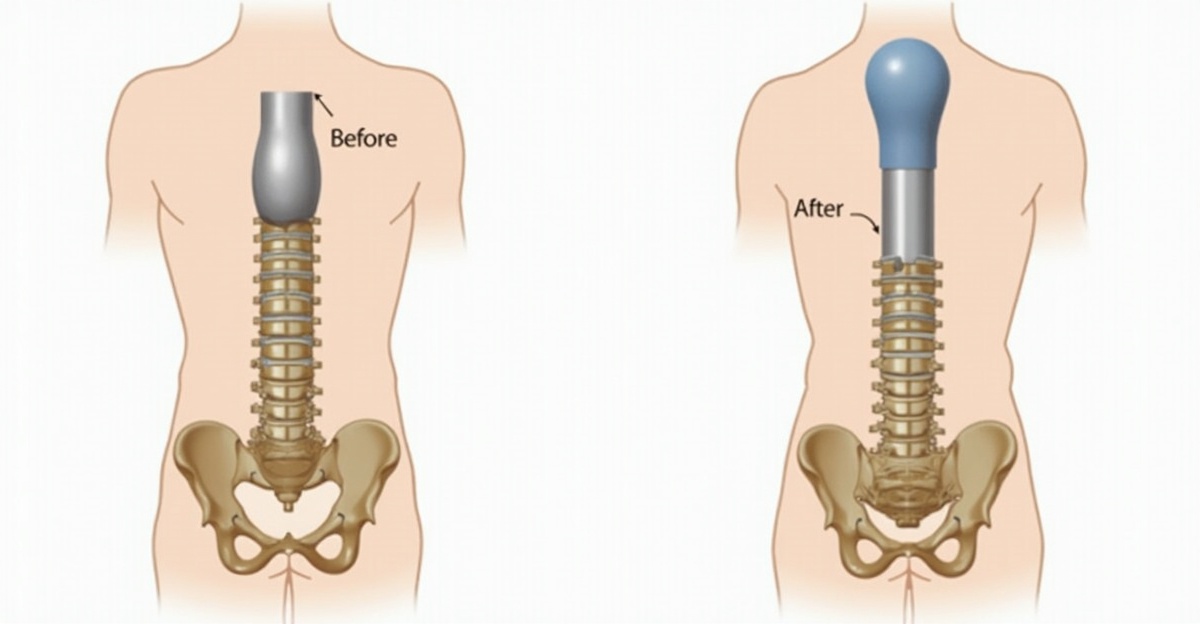
Balloon Kyphoplasty
Uses an inflatable balloon to create a cavity before cement injection, potentially restoring vertebral height and reducing kyphotic deformity.
- Lower cement leak rates
- May improve vertebral height
- Controlled cement placement
Vertebroplasty
Direct injection of bone cement into the fractured vertebra without balloon expansion. Typically shorter procedure time.
- Shorter operative time
- Less expensive procedure
- Similar long-term outcomes
Clinical Evidence: Head-to-head trials report similar long-term pain/disability outcomes; kyphoplasty tends to have fewer cement leaks and may improve vertebral height/kyphosis, while vertebroplasty is typically shorter.
Timing Matters: When to Intervene
The 4-Week Window
Earlier intervention (<4 weeks) after failed conservative care and imaging-confirmed acuity is associated with better pain/function in meta-analysis.
Acute Phase (0-4 weeks)
- Optimal timing for intervention
- Best height restoration potential
- Faster pain relief
Subacute (4-12 weeks)
- Still beneficial for pain
- Limited height restoration
- Case-by-case evaluation
Chronic (>12 weeks)
- Limited benefit expected
- Consider alternative treatments
- Focus on bone health
Key Cautions & Contraindications
Absolute Contraindications
Not for infection, unstable burst fractures, or untreated coagulopathy. Always pair with bone-health optimization.
- Active spinal infection (osteomyelitis)
- Unstable burst fractures with retropulsion
- Uncorrected bleeding disorders
- Severe spinal canal compromise
Essential: Bone Health Optimization
Kyphoplasty treats the fracture but doesn't address underlying osteoporosis. Comprehensive bone health management is crucial for preventing future fractures.
- Calcium and Vitamin D supplementation
- Bisphosphonate or other anti-resorptive therapy
- Fall prevention strategies
- Regular bone density monitoring
Outcomes & Realistic Expectations
Expected Benefits
- pain improvement that varies by patient (70-90% of patients)
- Improved mobility and function
- Reduced narcotic dependence
- Faster return to activities
Potential Risks
- Cement leakage (5-10% symptomatic)
- Adjacent level fractures
- Infection (rare, <1%)
- Incomplete pain relief
Related Topics
Learn more about related conditions and treatments
About this content
This page was written and clinically reviewed by Marc Greenberg, MD, a fellowship-trained spine surgeon who trained at Mayo Clinic, Johns Hopkins, and Brown University, practicing in Fort Wayne, Indiana. Information is for educational purposes only and is not a substitute for medical advice from your physician.
Suffering from a Compression Fracture?
Schedule a consultation to determine if kyphoplasty is right for your vertebral compression fracture.
Related Information
Disclaimer: Information is educational, not medical advice. Outcomes vary. Individual results depend on many factors including age, health status, anatomy, and adherence to post-operative instructions. Always consult with a qualified spine surgeon for personalized medical advice.
Related Articles

Minimally Invasive Spine Surgery: What Indiana Patients Should Know
A patient-friendly educational guide to minimally invasive spine surgery (MIS) for Indiana patients. Covers what MIS actually means (a spectrum of techniques using smaller incisions and muscle-sparing approaches to achieve the same surgical goal), how it differs from traditional open surgery (comparison table covering incision size, muscle handling, blood loss, hospital stay, post-operative discomfort, and visualization), common conditions treated with MIS (herniated discs, spinal stenosis, spondylolisthesis, compression fractures, and degenerative disc disease — all with the caveat that surgery follows conservative care trial), what recovery looks like across four phases (immediate post-op, first two weeks, weeks 2-6, and longer-term with warning signs to call about), and practical guidance for accessing MIS care in Indiana and Northeast Indiana including the importance of fellowship training and starting with a consultation. Includes FAQPage JSON-LD, internal links to MIS overview, procedures, and related blog posts.

How to Choose the Right Spine Surgeon in Fort Wayne, Indiana: What Patients Should Know Before Scheduling Surgery
Fellowship-trained Fort Wayne spine surgeon Dr. Marc Greenberg explains what patients should look for when choosing a spine surgeon in Fort Wayne: fellowship training at Mayo Clinic, Johns Hopkins, and Brown University, minimally invasive and endoscopic expertise, motion-preservation philosophy, robotic-assisted capabilities, peer-reviewed research, and an evidence-based approach. Includes red flags vs. green flags comparison, questions to ask before surgery, and why Fort Wayne patients no longer need to travel to Indianapolis or Chicago for world-class spine care.
Spondylolisthesis: What Indiana Patients Need to Know About Grades, Symptoms, and Treatment
An educational guide on spondylolisthesis for Indiana patients. Covers what spondylolisthesis means in plain terms (a vertebra slipping forward), the five-grade classification system with a clear table showing what each grade means and the typical approach, the different types (degenerative as the most common in adults over 50, isthmic from a stress fracture often in adolescent athletes, congenital, traumatic, and pathologic), how it is diagnosed (X-ray, MRI, dynamic flexion-extension views), symptoms (mechanical back pain and nerve-related leg symptoms — with the important note that many people have no symptoms at all), and the graduated treatment approach from conservative care through surgical fusion. Includes FAQPage JSON-LD, internal links to spondylolisthesis patient education, lumbar fusion, laminectomy, and related resources.